Risk factors of elderly patients with postoperative delirium following major abdominal surgery for cancer
Article information

Abstract
Purpose
Postoperative delirium (POD) is a common complication in elderly patients after major abdominal surgery for cancer. Although POD is related with a poor outcome, there have not been many reports about POD after abdominal surgery in Korea. The aims of study were to analyze the characteristics and surgical outcomes of elderly patients with POD and to identify the risk factors of POD.
Methods
From November 2016 to January 2019, we prospectively enrolled 63 patients who were aged ≥75 years and underwent major abdominal surgery for cancer. POD was daily assessed for up to 10 days postoperatively with the Confusion Assessment Method and a validated chart review.
Results
POD occurred in eight patients (12.7%). Univariate analysis showed that the occurrence of POD was related to sodium <135 mEq/L (P=0.037), combined resection (P=0.023), longer surgery/anesthesia time (P=0.023 and P=0.037, respectively), increased blood loss (P=0.004), postoperative admission to intensive care unit (ICU) (P=0.023), and duration of Foley catheter (P=0.011), however, multivariate analysis identified no significant risk factors of POD. There was no difference in postoperative outcomes such as hospital stay, mortality, reoperation, and morbidity between patients with POD and without POD.
Conclusion
Elderly patients with hyponatremia, combined resection, longer operation/anesthesia time and admission to ICU had tendencies to develop POD after major abdominal surgery. Surgeons should pay more attention to prevent POD, and a large-scale prospective study is needed to identify the risk factors of POD.
INTRODUCTION
The number of elderly patients undergoing major abdominal surgery is increasing. This trend will continue as life expectancy has improved and the population is aging. Understanding the risks for adverse outcomes in the aging surgical population is essential to increase safety and reduce costs. In elderly patients, delirium is known as the most common surgical complication with an incidence of 15% to 25% after major elective surgery and 50% after high-risk procedures such as hip-fracture repair and cardiac surgery [1]. Furthermore, a strong correlation has been observed between increasing age and incidence of postoperative delirium (POD) after major surgery [2]. The official diagnosis of delirium by Diagnostic and Statistical Manual of Mental Disorders (DSM-5) required following criteria: (1) disturbance in attention (i.e., reduced ability to direct, focus, sustain, and shift attention) and awareness (reduced orientation to the environment); (2) the disturbance develops over a short period of time (usually hours to a few days), represents an acute change from baseline attention and awareness, and tends to fluctuate in severity during the course of a day; (3) an additional disturbance in cognition; (4) the disturbances in criteria (1) and (3) are not better explained by a pre-existing, established, or evolving neurocognitive disorder and do not occur in the context of a severely reduced level of arousal such as coma; and (5) there is evidence from the history, physical examination or laboratory findings that the disturbance is a direct physiological consequence of another medical condition, substance intoxication or withdrawal, or exposure to a toxin, or is due to multiple etiologies [3]. POD is a potential risk factor for extended lengths of stay, higher patient care costs, morbidity, discharge to a post-acute nursing facility, and greater risk of death [4–6]. In Korea, there have been several reports on POD in patients after abdominal surgery, but most of them demonstrated POD in patients after liver transplantation [7–9]. The incidence of POD in elderly patients was reported as around 18.3% after major abdominal surgery [10], 8.6%–41.2% after gastrectomy [11,12], and 8.8% after colorectal surgery [12]. These differences in incidence were related with the methods for diagnosis of POD. Many studies in Korea were retrospective or observatory studies using chart review or big data, which had tendencies to underestimate the incidence of POD.
This prospective study aimed to identify the incidence of POD after major abdominal surgery for cancer and to analyze the risk factors and surgical outcomes of elderly patients with POD.
METHODS
Patients
From November 2016 to January 2019, we prospectively enrolled elderly patients who were aged 75 years and greater and underwent major abdominal surgery. Patients with delirium at admission, emergent surgery, severe visual disturbance, dementia, and aphasia were excluded. Patients who were discharged within 5 days were also excluded. This study was approved by the Institutional Review Board of Seoul Metropolitan Government Seoul National University Boramae Medical Center (IRB No. 16-2014-1023/091) and written informed consent was obtained.
Anesthesis, surgery, and postoperative course
General anesthesia was used in all patients. It was induced with intravenous (IV) administration of fentanyl, propofol, and rocuronium without premedication, and was maintained with sevoflurane. At the end of surgery, the residual neuromuscular blockade was reversed with IV injection of glycopyrrolate, pyridostigmine and/or sugammadex.
Surgical procedures were classified into four categories to assess the influence of each surgical procedure on the development of POD: (1) gastric surgery including partial or total gastrectomy; (2) colorectal surgery including colectomy and proctectomy; (3) hepatic surgery; or (4) biliary-pancreatic surgery. Laparoscopic surgery was frequently used except in patients presenting with low cardiopulmonary function or intraabdominal severe adhesion.
After surgery, all patients used IV patient-controlled analgesia using fentanyl and Aloxi in 100 mL of saline and/or morphine. The following were determined by the surgeons in charge; (1) postoperative admission to intensive care unit (ICU); (2) need to restrain of patients extremities; (3) date of removal of the nasogastric tube and Foley catheter; (4) date of restoration of a diet; or (5) discharge if no surgical or systemic complications occurred.
Assessment and treatment of preoperative mental status and POD
The presence of delirium was daily assessed for up to 10 days postoperatively with the Confusion Assessment Method (CAM) [13, 14], which has four criteria (acute onset and fluctuating course, inattention, disorganized thinking, and altered level of consciousness) and a validated chart review. When the patients were postoperatively admitted to the ICU, CAM-ICU was used [15]. All patients were seen at least once a day by a surgeon. Treatment of POD was monitored by a psychologist and was based on treatment of the eventual cause, and the administration of quetiapine. Antipsychotics medication such as haloperidol was avoided as much as possible since it could aggravate the severity and the duration of POD. Antipsychotic medication was only used to decrease the considerable agitation and aggressiveness observed in some patients with POD, who became dangerous to themselves and other caregivers.
Data collection
We collected preoperative data, anesthetic and surgical data and postoperative data.
Preoperative data included demography (gender, age, weight, height, education level, marital status, and heavy drinker) comorbidity, visual disturbance, the American Society of Anesthesiologists (ASA) classification, Eastern Cooperative Oncology Group performance status, preoperative cognitive function, activities of daily living using Barthel index, nutritional status, and laboratory test results. Cognitive function of the patients was assessed using the Mini-Mental State Examination-Korean (MMSE, score range of 0–30) the day before surgery and all tests were conducted independently by a trained research nurse. Nutritional status was performed using Mini-Nutritional Assessment (MNA), which is well known to be an accurate nutritional assessment tool and is highly correlated with both clinical assessments of nutritional status and objective indicators such as serum albumin [16]. Nutritional status was divided to normal (24–30), risk of malnutrition (17–23.5), and malnutrition. Laboratory investigations included serum hemoglobin levels, serum electrolyte levels, the serum albumin level, and the serum calcium level.
Anesthetic and surgical data included type of surgical procedure, operative time, anesthetic time, intraoperative hypotensive event, estimated blood loss, and intraoperative transfusion.
Postoperative data included duration of Foley catheter, restrain, postoperative ICU stay, hospital stay, morbidity, mortality and readmission. Postoperative morbidity was graded based on the Clavien-Dindo classification [17], and according to this grading, grade III, IV, and V complications were classified as major complications.
Statistics
Patients’ data were summarized using mean±standard deviation for continuous variables and frequency (%) for categorical variables. Continuous variables were compared using the two-sample t-test and/or Wilcoxon rank-sum test. Categorical variables were compared using Pearson chi-square test or the Fisher exact test. A Cox proportional hazard model analysis was performed to identify risk factors for the development of POD.
A two-sided P-value of <0.05 was considered statistically significant. Statistical analysis was performed using IBM SPSS version 23 (IBM Corp., Armonk, NY, USA).
RESULTS
Among 143 eligible patients, only 67 patients agreed to participate in this study and four patients were excluded (two withdrawal of consent and two aborted surgery after discovering peritoneal seeding). Finally, 63 elderly patients were included.
Patients’ preoperative characteristics were summarized in the Table 1. Mean age of patients was 79 years (range, 75–88 years). Body mass index of 10 patients (15.9%) was 20 kg/m2 and less, and the ASA classification of all patients was 2. The score MMSE of 29 patients (46%) was lower than 24.

Preoperative characters of elderly patients
POD was confirmed in eight patients (12.7%), of which five patients (62.5%) required antipsychotic medication. Seven patients (87.5%) were diagnosed with POD, which developed within 4 days after surgery and occurred during the first postoperative week.
According to univariate analysis, the occurrence of POD was related to sodium <135 mEq/L (P=0.037), combined resection (P=0.023), duration of surgery (P=0.023), duration of anesthesia (P=0.037), estimated blood loss (P=0.004), postoperative admission to ICU (P=0.023), and duration of Foley catheter (P=0.011) (Table 2). Multivariate analysis identified no significant risk factors of POD (Table 3).
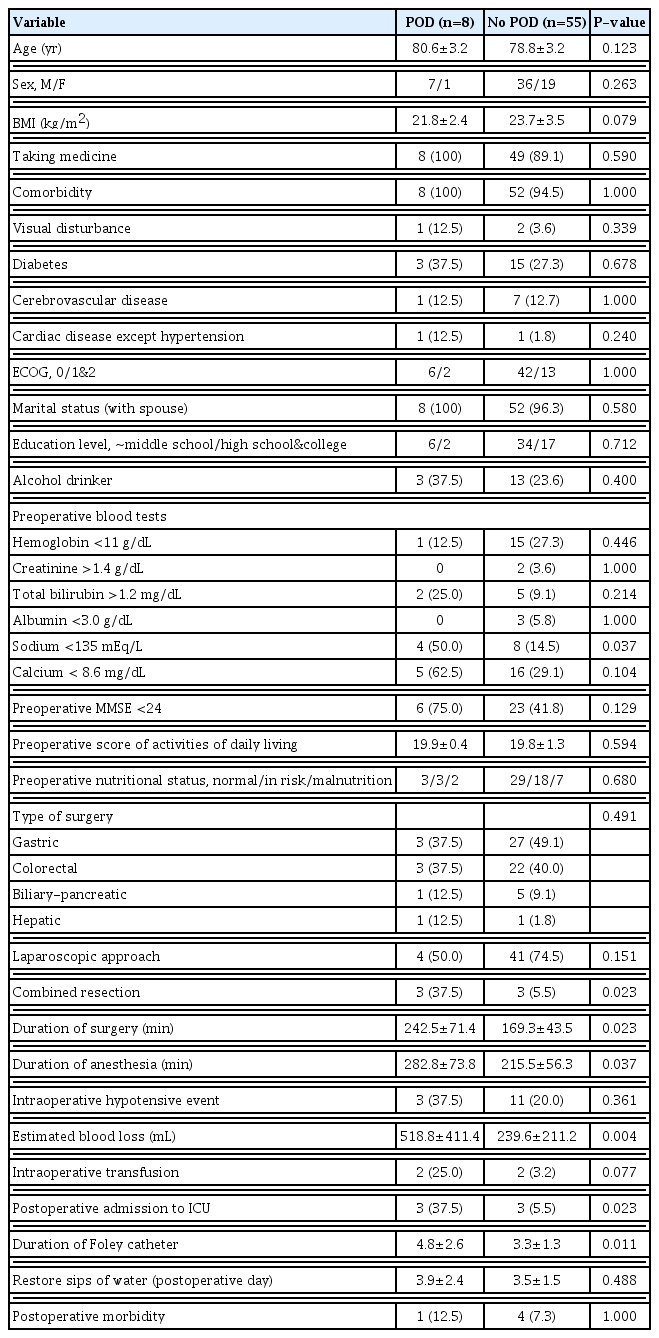
Risk factors for postoperative delirium in 63 elderly patients

Multivariate analysis of risk factors for postoperative delirium in 63 patients
Postoperatively, there was no reoperation and only one mortality in patients without POD. Eight patients with POD had similar hospital stay, 90-day mortality, reoperation and postoperative morbidity compared with 55 patients without POD (Table 4). The postoperative mean time to passage of flatus was 5.6±2.7 days in eight patients with POD and 4.7±2.6 days in 55 patients without POD (P=0.450). The postoperative mean time to being able to tolerate a solid diet was 5.1±2.3 in eight patients with POD and 4.9±1.8 in 55 patients without POD (P=0.757).
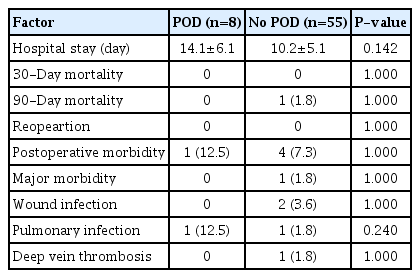
Surgical outcomes of 63 elderly patients according to POD
DISCUSSION
The incidence of POD was reported as an average 36.8% of surgical patients and varied from 9% to 87% depending on age, setting, type of surgery, other risk factors and the variation in screening practices [4,18]. Risk factors for POD have been categorized into predisposing and precipitating factors [4]. Older age, dementia (often not recognized clinically), functional disabilities, and a high burden of coexisting conditions are common predisposing factors. Male, poor vision and hearing, depressive symptoms, mild cognitive impairment, laboratory abnormalities, and alcohol abuse have also been known as predisposing factors [4]. On the other hand, drugs (especially sedative hypnotic agents and anticholinergic agents), surgery, anesthesia, high pain levels, anemia, infections, acute illness, and acute exacerbation of chronic illness are commonly reported precipitating factors [4]. Others reported that predictors of POD included delirium in medical history, advancing age per 10 years, ASA-score ≥3, impaired mobility (timed get up and go test score >20 seconds) and postoperative tramadol administration [2,6]. According to Dhakharia et al. [19], respiratory complications, ICU stay >24 hours were also significantly associated with the POD.
This prospective study identified the incidence of POD as 12.6% in elderly patients aged 75 years and greater following major abdominal surgery for cancer in Korea. However, this study failed to identify the risk factors for POD and the association with poorer surgical outcomes in patients with POD. This failure might come from relatively low postoperatively morbidity and the small number of patients.
POD is usually known to negatively affect the postoperative course of clinical recovery, length of hospital stay, patient care costs, morbidity, discharge to a post-acute nursing facility, and greater risk of death [4–6]. Furthermore, major postoperative complications and delirium can demonstrate a strong combined effect and they are separately associated with adverse events [5]. However, that 30% to 40% of cases of delirium are preventable [20] led to trials finding the effective interventions to prevent POD. Those trials included orienting communication, oral and nutritional assistance, and early mobilization [21,22]. The patients were underwent the comprehensive geriatric assessment and got nutritional assistance to improve patients’ preoperative health. Except these factors, surgeons have to do operation with good quality and short operative time to reduce the admission to ICU and postoperative pulmonary morbidity and surgeons should try not to use tramadol for the postoperative pain.
This study has several limitations. First, only 47% of eligible patients were included and this lowered the power of statistical analysis. The geriatric assessment included a large amount of inquiries and seemed burdensome. This could a hurdle in recruiting elderly patients. Second, the association between POD and the postoperative impairment of cognitive function could not be analyzed because the assessment of cognitive function was not postoperatively performed.
In summary, elderly patients with hyponatremia, combined resection, longer operation/anesthesia time, and admission to ICU had tendencies to develop POD after major abdominal surgery, although multivariate analysis failed to identify significant risk factors. Surgeons should pay more attention to prevent POD, and a large-scale prospective study is needed to identify the risk factors of POD.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
ACKNOWLEDGMENTS
This research was supported by Research Program 2015 funded by Seoul National University College of Medicine Research Foundation (800-20150342).