INTRODUCTION
Colorectal cancer (CRC) is the third most frequently diagnosed cancer in the world although almost a quarter of the cases (23%) are stage 1 [1]. In early CRC, treatment options include endoscopic procedures and surgical resection. Patients diagnosed early with CRC and little possibility of lymph node metastasis are initially treated by endoscopic procedures such as endoscopic mucosal resection and endoscopic submucosal dissection (ESD). However, patients at a high-risk for lymph node metastasis, including those with submucosal invasion depth ≥ 1,000 μm, poorly differentiated adenocarcinoma, lymphovascular invasion, and positive lateral and/or vertical resection margins, should be surgically treated with a radical lymphadenectomy [2].
Laparoscopic colorectal resection has become an alternative standard procedure for treating colorectal diseases, including malignant tumors [3]. Several prospective randomized control trials and meta-analyses on laparoscopic surgery for CRC have demonstrated that laparoscopic surgery is superior to open surgery in terms of improved perioperative outcomes such as lesser pain, smaller incision, faster recovery of gastrointestinal function, and shorter hospital stay [4–7]. In addition, studies comparing endoscopic treatment and laparoscopic surgery for early CRC have been published. However, more data are needed regarding the long-term oncologic outcomes between these two minimally invasive treatments. Therefore, this study aimed to compare the clinical and long-term oncologic outcomes between endoscopic procedures and laparoscopic surgeries in patients who were treated for early CRC.
METHODS
Patients and data collection
Data on patients treated between January 2010 and December 2013 were collected from the departments of gastroenterology and colorectal surgery at the study site. In total, 60 patients who underwent an endoscopic procedure for T1 colorectal adenocarcinoma and 38 patients who underwent laparoscopic surgery for T1N0M0 colorectal adenocarcinoma were enrolled. The exclusion criteria included synchronous or previous malignancies, malignancies other than adenocarcinoma, and cancer related to familial adenomatous polyposis or hereditary nonpolyposis CRC. The study protocol was approved by the Institutional Review Board of the Keimyung University Dongsan Medical Center (IRB No. 2020-07-097) and informed consent was obtained from all patients.
Using retrospective data collection, information on patient demographics included age, sex, preoperative carcinoembryonic antigen, body mass index, and location of the tumor. The perioperative details of the endoscopic procedure included the type of procedure, depth of invasion, margin status, and morbidity after endoscopic resection. The laparoscopic surgery outcomes included the type of operation, the number of harvested lymph nodes, and morbidities after surgery. Clinicopathologic comparative outcomes included operation time, recovery, mortality, tumor stage, histology, tumor size, and lymphovascular invasion. Oncologic outcomes included overall survival (OS) rate and disease-free survival (DFS) rate and recurrence pattern.
Indication of endoscopic treatment and laparoscopic surgery
The indications for endoscopic resection of the colorectal neoplasia in our institution are: (1) colorectal neoplastic lesion which was not suspected to be a deep submucosal invasive cancer based on white-light endoscopy and chromoendoscopy and (2) a laterally spreading tumor defined by flat neoplastic lesions that are 10 mm in size or larger and extending laterally and circumferentially, rather than vertically [8]. When the lesion was suspected to be a deep submucosal (sm2) invasive cancer based on endoscopic features such as loss of lobulation, expansive appearance, surface ulceration, surrounding convergent folds, or signs of non-lifting, endoscopic resection was not performed [9,10].
After endoscopic resection, patients with high-risk factors for recurrence chose surgical treatment or regular follow-up at a multidisciplinary clinic after endoscopic resection was done (Fig. 1).
Endoscopic technique
Endoscopic resections were performed by three expert endoscopists who have over 8 years of experience in therapeutic endoscopy. All procedures were performed with a single-channel endoscope (GIF-H260, GIF-Q260J; Olympus Co., Tokyo, Japan) and electrosurgical unit (VIO300D; ERBE, Tübingen, Germany). According to the institutional protocol, two types of endoscopic resections were applied for early colorectal cancer (ECC) as follows: ESD alone and ESD with snaring (ESD-S). The decision to perform ESD alone or ESD-S was made by the individual endoscopist, based on the ESD guidelines for CRC [11].
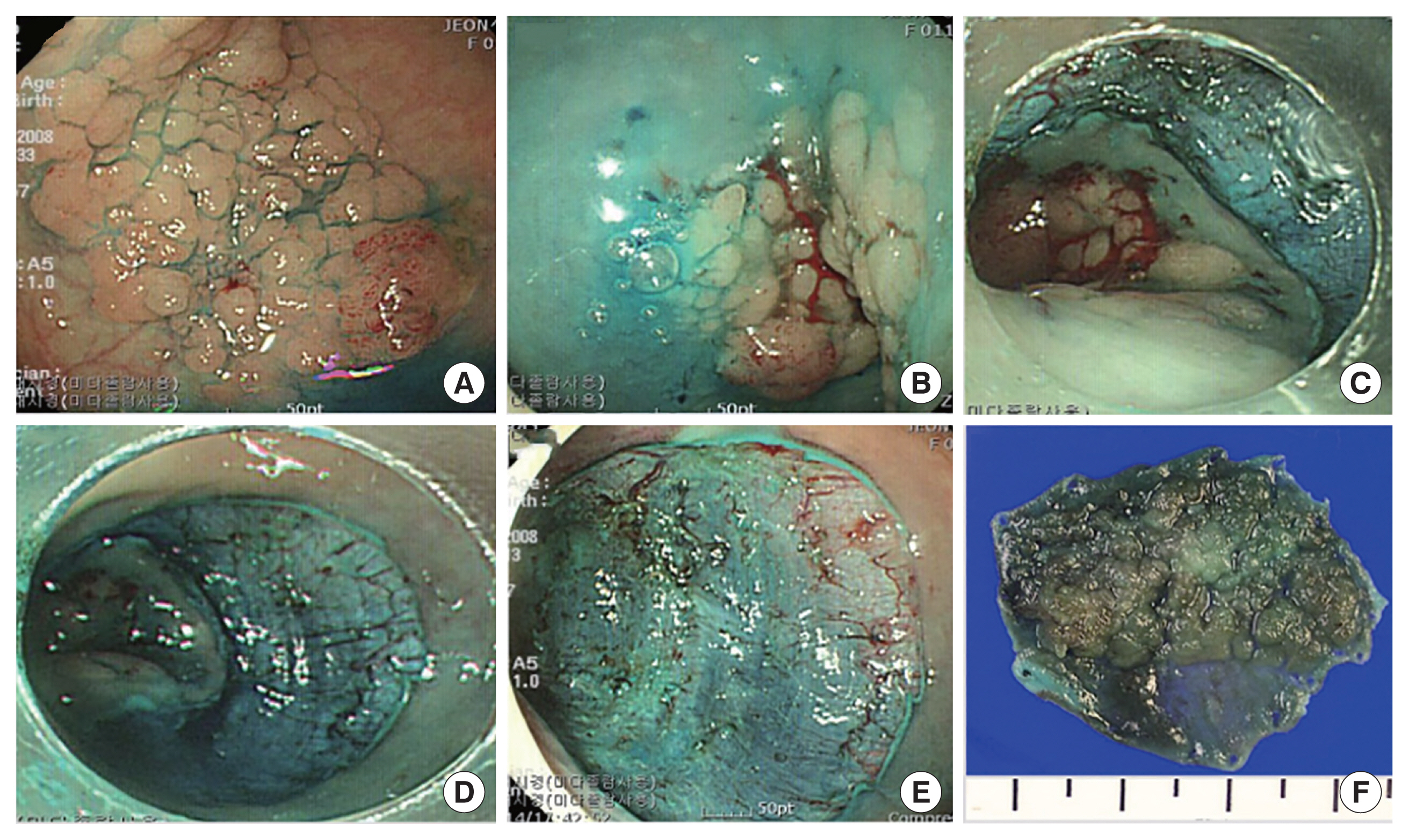
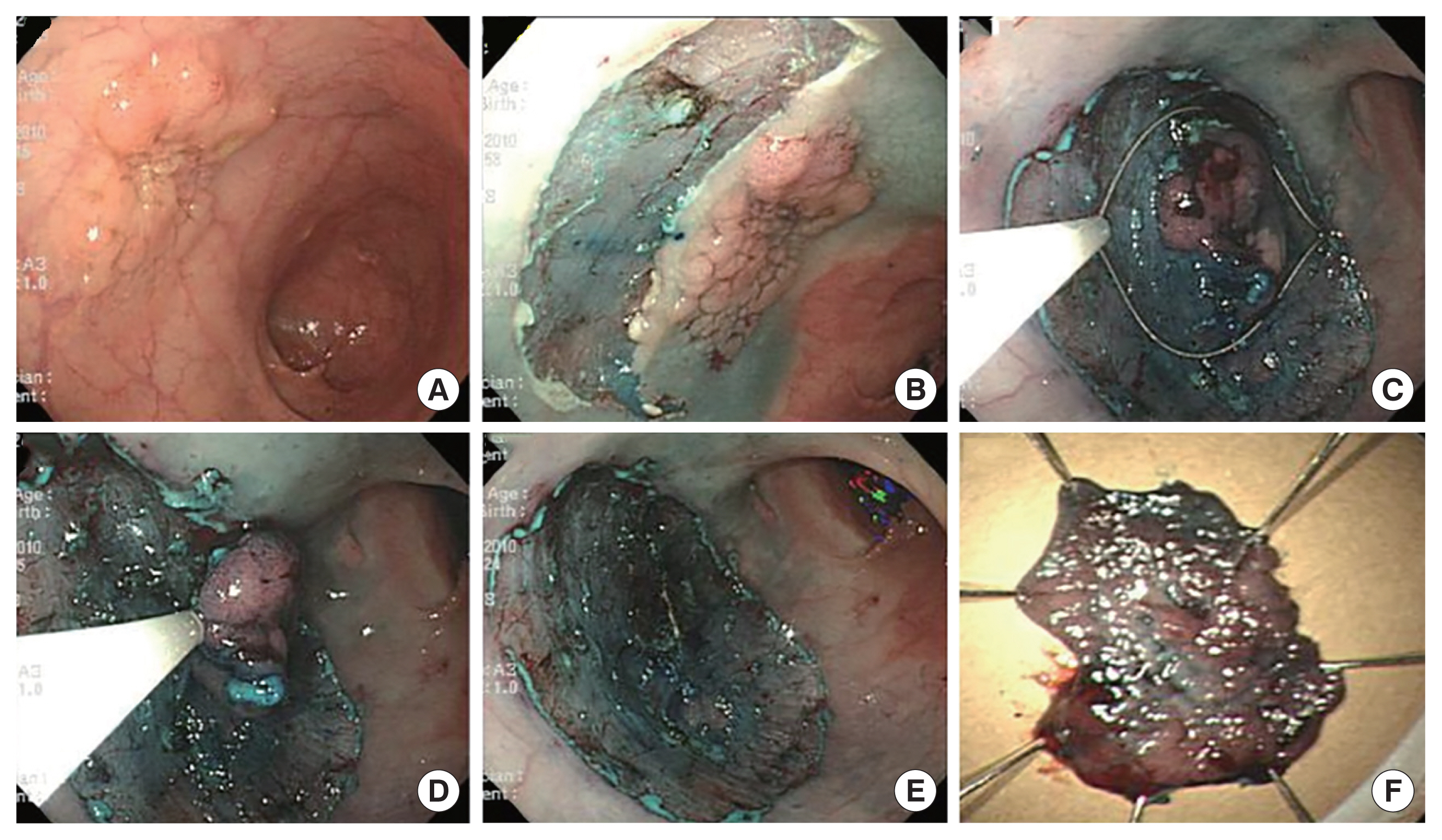
For ESD, the mucosa around the tumor was incised with a dual knife (Dual Knif; Olympus Co.) at a 2–3 mm periphery from the lesion to create a tumor-free lateral resection margin after the submucosal injection (Figs. 2, 3). Most of the submucosal dissection was performed with the dual knife alone, but in some cases, a hook knife (Hook Knife; Olympus Co.) was also used. For ESD-S, resection of the remnant undissected tissue was snared when there was insufficient primary submucosal dissection.
Laparoscopic technique
The laparoscopic surgeries followed the general principles of complete mesocolic excision and total mesorectal excision with central vascular ligation for CRC as previously described [11]. The primary tumor was interfaced by sharp dissection between the visceral plane and the parietal fascia layer along with the entire regional mesocolon and mesorectum in an intact package. We used 5 ports: two 12-mm ports for a camera (umbilicus) and a working port (above the umbilicus, left side, midclavicular line) and another three 5-mm ports in each remaining quadrant.
Statistical analysis
The results are presented as medians with ranges for continuous outcomes, and as frequencies with percentages for categorical outcomes. Categorical variables were analyzed using chi-square and Fisher exact tests. Continuous variables were analyzed with the independent t-test and Mann-Whitney test. The Kaplan-Meier method and log-rank test were used for survival analysis. Recurrence was defined as the presence of a radiologically confirmed or histologically diagnosed tumor. The location of recurrence was defined as the first site of recurrence after complete resection. Local recurrence was defined as any tumor recurrence in the surgical field. OS was defined as the time from the date of surgery to the date of the latest follow-up visit or the date of death due to any cause. DFS was defined as the time from surgery to any type of recurrence. A P-value of<0.05 was considered to indicate statistical significance. The statistical analyses were performed with SPSS version 25.0 software (IBM Corp., Armonk, NY, USA).
RESULTS
Baseline characteristics
There was no statistical difference between the two treatment groups according to age, sex, or preoperative carcinoembryonic antigen levels. Body mass index was statistically higher in the laparoscopic group than in the endoscopic group (25.1 kg/m2 vs. 24.4 kg/m2, P=0.050) (Table 1). Tumors tended to be more frequent in the rectum of patients in the endoscopic group and in the sigmoid colon the laparoscopic group (P=0.093).
Operative outcomes of endoscopic treatment
Operative outcomes of endoscopic treatment are described in Table 2. In total, 25 patients (41.7%) underwent ESD and 35 patients (58.3%) underwent ESD-S. There were 29 (48.3%) tumors invading the muscularis mucosa and 31 (51.7%) tumors invading the submucosa. Thirteen tumors (21.7%) invaded deeper than 1 mm and 16 tumors (26.7%) involved the surgical margin. After endoscopic treatment, there were three cases with bleeding (5.0%), six cases with perforation (10.0%), and two cases with bleeding and perforation (3.3%). Among the three patients who had post-procedure bleeding, two patients underwent coagulation during the procedure and one patient was observed with conservative management. Four patients with post-procedure perforation were treated by clipping during the procedure and the others recovered after conservative management. Among the two patients who had bleeding and perforation simultaneously during the endoscopic procedure, one patient was treated using hemo-clipping and the other patient was converted to the surgical treatment.
Operative outcomes of laparoscopic surgery
Operative outcomes of laparoscopic surgery are provided in Table 3. The most frequently performed procedure was 13 right hemicolectomies (32.2%) and the median number of retrieved lymph nodes was 19 (range, 3–49). Six patients had morbidities within 30 days after surgery including anastomotic site bleeding, chyle leakage, ileus, pseudomembranous colitis, difficulty voiding, and wound infection. One patient who had anastomotic site bleeding was treated with argon plasma coagulation via sigmoidoscopy. The patient with chyle leakage and ileus was managed with conservative management. There were no severe complications that required reoperation and no conversion to open surgery occurred.
Clinicopathologic outcomes
The clinicopathologic outcomes of the two treatment groups are summarized in Table 4. The median operation time was significantly longer for the laparoscopic group (187.5 minutes vs. 35.8 minutes, P<0.001). Time to sips of water and length of hospital stay were significantly shorter in the endoscopic group compared to the laparoscopic group (5 days vs. 1 day, P<0.001; 7 days vs. 2 days, p<0.001, respectively). The mean tumor size was larger in the endoscopic group compared to the laparoscopic group (1.5 cm vs. 1.8 cm, P=0.016) and the ratio of moderate and poorly differentiated lesions was significantly higher in the laparoscopic group compared to the endoscopic group (P=0.018). There was no significant difference between tumor stage or lymphovascular invasion between the two groups. Two patients who were treated for T1 cancer were finally diagnosed as stages T3 and T4 after endoscopic resection.
Oncologic outcomes and recurrence patterns
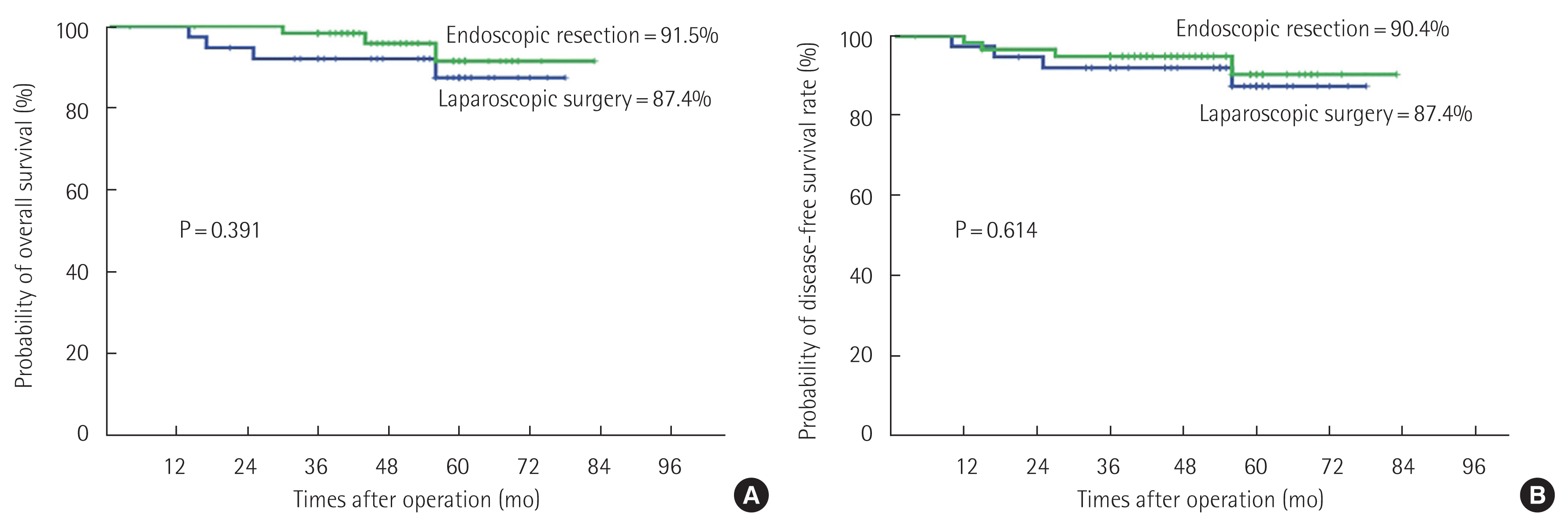
The median follow-up period was 56 months in the laparoscopic group and 50 months in the endoscopic group (Table 5). The OS rate was not significantly different between groups (87.4% in the laparoscopic group and 91.5% in the endoscopic group, P=0.391) (Fig. 4A). The DFS rates were 87.4% in the laparoscopic group and 90.4% in the endoscopic group (P=0.614) (Fig. 4B). There was no local recurrence in either group. Table 6 summarizes the cases of four patients with recurrence according to treatment type. There were three systemic recurrences in the liver (laparoscopic group: n=1 [2.6%], endoscopic group: n=2 [3.3%]). One rectal cancer patient who underwent an endoscopic procedure had local recurrence and systemic recurrence in the liver and lungs (0.8%).
After endoscopic treatment for early CRC, 32 patients had more than one high-risk factor (Fig. 1). After a multidisciplinary team approach, 17 patients (28.3%) underwent additional surgery due to high-risk factors and 15 patients did not undergo additional surgery due to old age and/or severe co-morbidities. Table 7 shows the details from patients who did not undergo additional surgery despite high-risk factors after endoscopic resection. Two patients were treated with chemoradiotherapy or chemotherapy and three patients underwent repeated endoscopic resection. Three patients were treated with repeated endoscopic procedures including ESD or ESD-S and 10 patients had regular follow-up without further treatment. Among the patients who underwent endoscopic re-resection, there was one systemic recurrence in the lungs 1 year after ESD.
DISCUSSION
This study aimed to compare endoscopic and laparoscopic outcomes for early CRC treatment to clarify clinical decision-making. Results of the present study show that patients who underwent endoscopic treatment had superior short-term clinical outcomes, including shorter operating time and hospital stay, and similar long-term oncologic outcomes compared to those who underwent laparoscopic surgery. Therefore, we recommend an endoscopic treatment as an initial intervention for early CRC with multidisciplinary approach.
As endoscopic techniques develop, there are attempts to expand the indications for this approach, including ESD, to treat early CRC with various techniques [12]. However, more evidence is needed regarding the short-term clinical outcomes between endoscopic and laparoscopic interventions for treating early CRC and comparative studies with long-term oncologic outcomes between the two groups are lacking [13,14]. Kiriyama et al. [14] reported that en bloc and curative resection rates for endoscopic and laparoscopic interventions were 87% and 80%, respectively. In the same study, the rate of post-procedure morbidities, including perforations and bleeding after endoscopic procedures, was 6.4% and in the laparoscopic group, the mean operation time was 206 minutes and the rate of complications including surgical site infection, pelvic abscesses, anastomotic leakages, and anastomotic bleeding was 12.6%. Inoue et al. [13] demonstrated that en bloc and curative resection rates were 93.7% and 87.4%, respectively, for endoscopic and laparoscopic interventions and complication rates were 8.4% during 5 days of hospital stay in the ESD group. In the laparoscopic surgery group, operative times were 228 minutes and the average hospital stay was 9 days with a 5.4% postoperative complication rate. In the present study, the operation time, time to sips of water, and hospital stay were shorter in the endoscopic group compared to the laparoscopic group with similar complication rates. These data support previous studies that demonstrate the feasibility and minimally invasive nature of endoscopic resection.
In a multicenter study that demonstrated the clinical and long-term outcomes of endoscopic treatment reported that the DFS and recurrence rates of early CRC in patients with low-risk factors, such as well to moderately differentiated, ≥ 2 mm cancer-free margin, and Haggitt invasion level 1–3, were 98% and 0.8%, respectively, whereas the rates in patients with high-risk factors were 89% and 6.6%, respectively [15]. Ikematsu et al. [16] also reported that overall recurrence-free survival rates and recurrence rates were 96% and 0% for patients with colon cancer and 90% and 6.3% for rectal cancer, respectively. In a high-risk group, recurrence-free survival rates and recurrence rates were 96% and 1.4% for colon cancer and 77% and 16.2% for rectal cancer patients, respectively [16]. In the present study, the DFS and recurrence rates were 90.4% and 4.1%, respectively, in the endoscopic group. Among the patients in this group, 32 patients (53.3%) were identified as high-risk and 17 of these patients were referred to the surgical department for radical resection. As a result, there was no recurrence in these patients, providing evidence for the long-term oncologic safety of endoscopic resection with salvage surgery for ECC.
The 15 patients who refused a radical resection despite a recommendation in the present study, cited old age and co-morbidities as the reason. Among these patients, five patients were treated with chemotherapy, chemoradiation, or endoscopic re-resection. There was one systemic recurrence in the lungs one year after re-ESD. The tumor was a moderately differentiated tubular adenocarcinoma with submucosal 3 mm invasion and suspected angiolymphatic invasion. Based on our study, surgical resection could be recommended after the identification of high-risk factors after endoscopic treatment, although careful observation of patients with co-morbidities and/or old age is also recommended.
Several multicenter prospective studies have demonstrated the feasibility and safety of laparoscopic surgery for CRC and this surgical approach has become the technique of choice for performing CRC resection [17,18]. In the present study, short-term outcomes of laparoscopic surgery including the time to oral feeding, length of hospital stay, and operation time were comparable to previous studies. Regarding the long-term outcomes, the one study reported that the 5-year survival rates were about 80% and recurrence rates were 8% for stage I CRC in laparoscopic groups [17]. In the present study, the OS rates were 87.4% and recurrence rates were 2.6% in the laparoscopic patients, demonstrating the long-term oncologic safety of laparoscopic surgery.
There are some limitations to the current study including its retrospective nature, selection bias, small sample size, and single-center study. However, this study adds to the literature by providing evidence for the evaluation of long-term oncologic outcomes between two minimally invasive treatments.
In conclusion, endoscopic resection for early CRC can be performed safely with better short-term clinical outcomes and similar long-term oncological outcomes compared to laparoscopic surgery. We recommend an endoscopic treatment as an initial intervention for early CRC with multidisciplinary approach.